Non-surgical treatment resolves coccyx pain (coccydynia) in approximately 80–90% of cases. The right combination of coccyx cushions, targeted physiotherapy, anti-inflammatory strategies, and ergonomic modifications can eliminate tailbone pain without ever needing a surgical consultation. This guide covers every evidence-based option — and how to prioritise them.
Last updated: April 2026 | Author: Mat | Read time: 18 minutes

The Coccyx Relief System — Everything You Need in One Place
Exercises, ergonomic setups, stretches, and a complete daily program. 30+ pages, instant download.
Get My Coccyx Relief SystemInstant download • 30-day money-back guarantee
Table of Contents
- Understanding Coccyx Pain: Why Sitting Hurts
- Home Remedies: Your First Line of Defence
- The Coccyx Cushion: The Single Most Important Investment
- Physiotherapy: The Gold Standard Non-Surgical Treatment
- Medications and Injections
- Ergonomic and Lifestyle Modifications
- Alternative and Complementary Therapies
- When Surgery Becomes Necessary
- Recovery Timeline: What to Expect
- Frequently Asked Questions
- Sources & Methodology
Understanding Coccyx Pain: Why Sitting Hurts
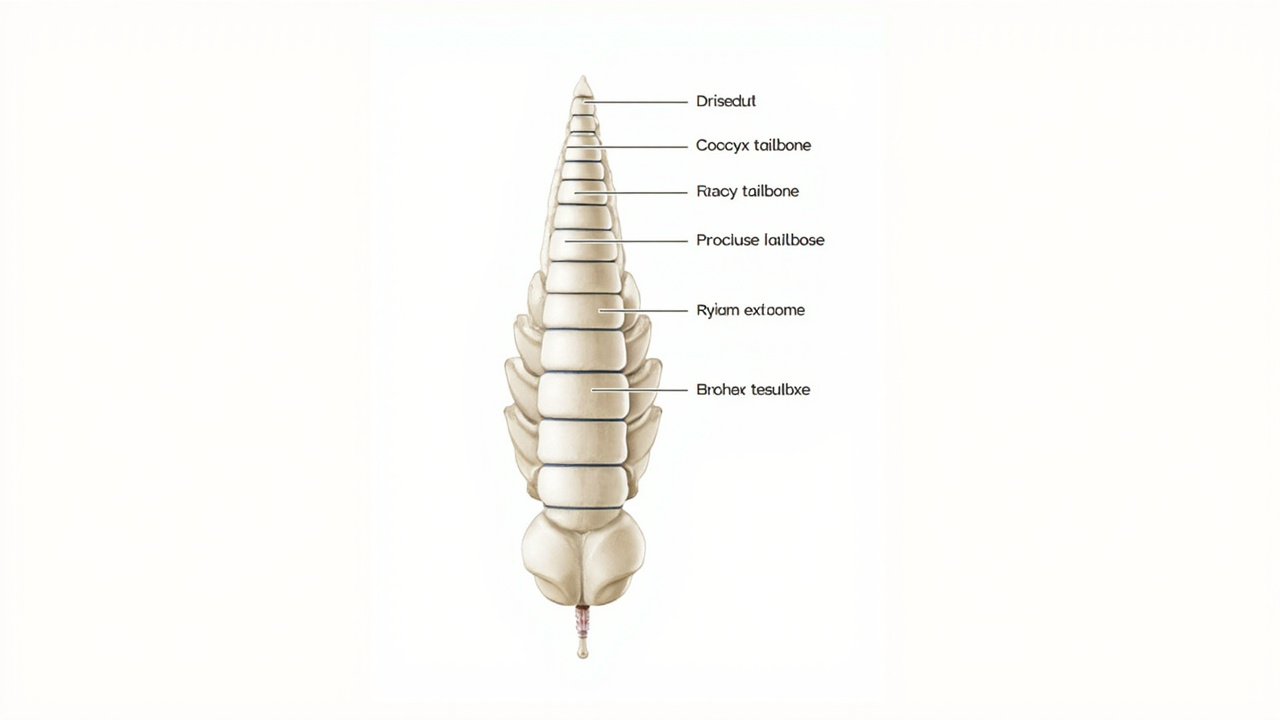
The coccyx — your tailbone — is the final 3–5 fused vertebrae at the base of your spine, sitting just below the sacrum. Despite its small size, it carries significant functional importance: it is an attachment point for the gluteus maximus muscle, multiple ligaments of the pelvic floor, and the anococcygeal raphe. Together, these structures stabilise the pelvis during sitting and help distribute weight through the pelvic floor.
Coccydynia is the medical term for pain in and around the coccyx. It is characterised by:
- Localised tenderness directly over the tailbone
- Pain worsened by sitting, particularly on hard surfaces
- Pain when transitioning from sitting to standing ("the stand-up wince")
- Pain during bowel movements or sexual intercourse
- Aching or throbbing at the base of the spine after prolonged sitting
Common Causes of Coccyx Pain
Trauma is the most common cause. A direct fall onto the tailbone — common from slipping in bathrooms, falling off bicycles, or landing on hard floors — can bruise, dislocate, or fracture the coccyx. Unlike most fractures, coccyx fractures are rarely immobilised; they heal with rest and conservative management.
Childbirth places enormous pressure on the coccyx. During vaginal delivery, the coccyx naturally moves backward to widen the pelvic outlet. In difficult or prolonged deliveries, especially with forceps or ventouse assistance, the coccyx can fracture or become significantly displaced. This is one of the most underreported postpartum injuries, affecting an estimated 10–20% of women after vaginal delivery. Our detailed guide on coccyx pain after childbirth covers this topic separately.
Prolonged sitting on poorly designed seating is an increasingly prevalent cause in modern life. The coccyx bears the brunt of body weight when seated on hard surfaces, and over time this repetitive pressure causes inflammation in the sacrococcygeal joint even without a specific injury.
Joint hypermobility or hypomobility in the sacrococcygeal joint can cause pain independently or following injury. Hypermobility allows excessive movement that irritates surrounding nerves; hypomobility (a stuck joint) causes mechanical pain with every movement.
Degenerative changes in the sacrococcygeal joint are common with ageing and may cause chronic pain even without a specific triggering event.
Why Coccyx Pain Is Frequently Misdiagnosed
Coccydynia is regularly misdiagnosed or overlooked because:
- Imaging (X-ray, MRI) often appears normal even in genuine cases
- Many clinicians do not routinely examine the coccyx
- Pain is located in a sensitive area patients may be reluctant to discuss
- Referred pain from the sacroiliac joint, lumbar spine, or pelvic floor can mimic coccyx pain
- Sciatica (pain radiating along the sciatic nerve) can cause referred pain in the tailbone region, leading patients to pursue treatments for sciatica while the underlying coccyx issue goes unaddressed — see sciaticaspot.com for a comprehensive guide to sciatica symptoms, causes, and treatment
A proper assessment by a pelvic physiotherapist or coccyx-specialist doctor includes internal palpation of the sacrococcygeal joint — something most general practitioners do not perform. If you have had coccyx pain for more than 8 weeks without a proper manual assessment, seek a specialist.
Home Remedies: Your First Line of Defence
Before spending money on physiotherapy sessions or medical interventions, there are several home remedies that meaningfully reduce coccyx pain for most people.
Ice and Heat Therapy
Ice (first 72 hours after injury or flare-up): Apply an ice pack wrapped in a thin cloth directly over the tailbone for 15 minutes at a time, 3–4 times daily. Ice reduces acute inflammation and numbs nerve endings. Never apply ice directly to bare skin — this can cause skin damage.
Heat (after the first 72 hours): Switch to a heat pack, warm bath, or hot water bottle. Heat relaxes the surrounding gluteal and pelvic floor muscles, improves blood flow to the area, and reduces the muscle guarding that develops in response to coccyx pain. Many people find heat more effective than ice even in the early stages once initial inflammation has settled.
Contrast therapy: Some patients find alternating ice and heat (15 minutes ice, 15 minutes heat, 2–3 cycles) most effective for chronic coccydynia. The thermal contrast promotes circulation and reduces muscle tension.
Sitting Posture Modifications
The single most important home modification is eliminating direct coccyx pressure during sitting. This means:
- Never sit on hard surfaces (kitchen chairs, wooden benches, concrete)
- Sit only on a coccyx cushion (see next section)
- Lean forward slightly when sitting — this shifts weight onto the ischial tuberosities ("sit bones") rather than the coccyx
- Avoid slumping, which places more pressure on the tailbone
- Take a 5-minute break every 30–45 minutes of sitting to allow pressure to redistribute
Donut Cushions (Standard)
For short-term acute relief — such as immediately after a fall or during a flare-up — a standard inflatable or foam donut cushion can help by distributing pressure away from the coccyx. However, donut cushions are inferior to U-shaped coccyx cushions for prolonged use because they still place some pressure on the perineal area and do not fully offload the tailbone.
Standing Desk and Movement Breaks
If your coccyx pain is aggravated by desk work, a standing desk or sit-stand workstation is one of the most effective investments you can make. Alternating between sitting (on a coccyx cushion) and standing every 30–45 minutes prevents prolonged pressure on the coccyx and reduces cumulative daily loading.
Even without a standing desk, the habit of standing up and walking for 2–3 minutes every half hour makes a meaningful difference. Setting a phone or computer reminder is an effective behaviour change strategy.
Sleeping Position Modifications
Coccyx pain disturbs sleep for many patients. To reduce tailbone pressure while sleeping:
- Side sleeping with a pillow between the knees reduces pressure on the sacrum and coccyx
- Back sleeping with a small pillow or rolled towel under the knees takes load off the lower back
- Avoid stomach sleeping — this position places the coccyx under pressure from the mattress and forces the lumbar spine into excessive extension
The Coccyx Cushion: The Single Most Important Investment
A coccyx cushion is not a luxury — it is the single most effective non-surgical intervention for coccyx pain. For anyone who sits for more than 2 hours per day with coccydynia, it is non-negotiable.
Why a Coccyx Cushion Works
When seated on a standard chair, your body weight is distributed across the entire contact surface — including the coccyx. A coccyx cushion with a U-shaped rear cutout completely removes the coccyx from the weight-bearing surface. Your weight instead distributes across the thighs and the area around (but not over) the tailbone.
This offloading allows the inflamed sacrococcygeal joint and surrounding soft tissues to rest and heal, rather than being continuously aggravated during sitting.
What to Look for in a Coccyx Cushion
U-shaped rear cutout (not a notch): A genuine U-shaped cutout — not just a shallow indentation — is essential. Many cheap "coccyx cushions" on Amazon have a notch rather than a true cutout and provide minimal coccyx offloading. The cutout should be at least 2 inches deep from the rear edge.
High-density memory foam: Standard foam flattens quickly with daily use. High-density memory foam (50–65 kg/m³) maintains its shape over years of use. Test this by pressing firmly with your thumb — quality foam should indent slowly and recover quickly.
Minimum 3-inch thickness: Thinner cushions bottom out on firm surfaces, eliminating the benefit. 3 inches or more ensures the coccyx stays clear of the seating surface even on hard chairs.
Ergonomic design: Look for a slight wedge shape (thicker at the back) which encourages a natural anterior pelvic tilt and reduces lower back strain.
Washable, breathable cover: A removable, machine-washable cover is essential for daily use. A mesh or perforated cover keeps you cooler during extended sitting.
Top Recommended Coccyx Cushions
Everlasting Comfort Seat Cushion — Our top overall pick. High-density memory foam that genuinely does not bottom out, a deep U-shaped rear cutout, non-slip bottom, and a machine-washable cover. Available on Amazon with the tag=theforge05-20. Check current price on Amazon.
ComfiLife Gel Enhanced Seat Cushion — The best option for people who run warm or live in hot climates. The cooling gel layer prevents the heat buildup that makes foam cushions uncomfortable during long sitting sessions. Check current price on Amazon.
Aylor Coccyx Seat Cushion — Excellent value mid-range option. Deep cutout, dense foam, and a washable cover. A reliable choice if you want quality without the premium price. Check current price on Amazon.
Putnams Coccyx Wedge — A wedge-shaped design rather than a flat cushion. Used extensively by NHS physiotherapists in the UK. The wedge shape promotes better pelvic alignment for some users, though the steeper angle may not suit everyone. Check current price.
Practical tip: Buy two — one for your primary desk or car chair, and one as a portable option for travel, office, or visiting friends and family. Carrying a cushion between locations is impractical and most people stop using them.
Portable Coccyx Cushions for Car and Travel
If you drive regularly or travel, a portable coccyx cushion is essential for car seats, airplane seats, and hotel chairs. Look for:
- A carrying handle or strap
- Removable, washable cover
- At least 2.5 inches of thickness despite the compact design
The Aylor and Everlasting Comfort both offer carry-handle models. Many users keep a permanent cushion in the car and use a separate one at their desk.
Physiotherapy: The Gold Standard Non-Surgical Treatment
Physiotherapy — specifically physiotherapy that includes manual coccyx mobilisation — is the most evidence-based non-surgical treatment for coccydynia. Multiple clinical studies report meaningful pain reduction in 60–80% of patients receiving manual coccyx treatment.
What a Coccyx Physiotherapist Does
A specialist pelvic floor or musculoskeletal physiotherapist will:
1. Assess the coccyx. This involves both external and (with your consent, for appropriate patients) internal palpation of the sacrococcygeal joint to determine whether the coccyx is hypermobile, hypomobile (stuck), or in a displaced position.
2. Perform manual coccyx mobilisation. If the joint is stuck or displaced, the physiotherapist applies gentle manual pressure — either externally through the gluteal cleft or internally — to restore normal joint motion. This is the technique most associated with clinical improvement in coccydynia research.
3. Address surrounding soft tissue restrictions. The gluteus maximus, piriformis, and pelvic floor muscles frequently develop secondary tension in response to coccyx pain. Manual release of these structures reduces referred pain and improves pelvic mechanics.
4. Prescribe targeted exercises. Beyond manual treatment, your physiotherapist will prescribe specific exercises to address your particular presentation — typically a combination of pelvic tilts, stretching, and core stability work. For those wanting to go deeper, our guide to pilates for coccyx pain covers how structured exercise complements physiotherapy.
5. Provide ergonomic advice. Your physiotherapist should give specific sitting, standing, and sleeping modifications tailored to your daily activities and occupation.
What to Expect at Your First Appointment
A thorough coccyx assessment typically takes 45–60 minutes for the initial consultation. You can expect:
- Discussion of your history: when the pain started, what aggravates it, previous treatments tried
- Observation of your posture, pelvic alignment, and gait
- Palpation of the lower spine, sacrum, and surrounding musculature
- Assessment of the sacrococcygeal joint (external and possibly internal)
- Functional movement assessment
- Development of a treatment plan
Internal examination of the coccyx is standard for patients with chronic coccydynia and requires informed consent. It is not painful but may feel uncomfortable. If you are not comfortable with internal examination, discuss this with your physiotherapist — external treatment approaches exist, though they are somewhat less targeted.
How Many Sessions Are Needed?
The number of sessions varies depending on the cause, severity, and duration of your coccyx pain:
- Acute injury (within 6 weeks): 3–6 sessions typically sufficient
- Post-childbirth coccydynia: 4–8 sessions, often combined with broader postpartum pelvic rehabilitation
- Chronic coccydynia (more than 6 months): 8–12 sessions, sometimes more
- Post-surgical rehabilitation: Individualised, typically 12+ sessions over 3–6 months
Most patients notice meaningful improvement within 3–4 sessions. If you have completed 6 sessions with no measurable improvement, ask your physiotherapist to reassess the diagnosis or consider a second opinion.
Ready to Actually Fix This? Don't Guess — Follow the System.
Stop trying random stretches. This is the exact step-by-step approach that works.
Get My Coccyx Relief SystemInstant download • 30-day money-back guarantee
Medications and Injections
Oral Pain Relief
NSAIDs (non-steroidal anti-inflammatory drugs): Ibuprofen, naproxen, and diclofenac reduce inflammation at the sacrococcygeal joint. They are most effective in the acute phase when inflammation is a primary driver of pain. Long-term daily use carries risks (gastrointestinal, cardiovascular, kidney function) and should be discussed with your GP.
Paracetamol: Less effective for inflammation but useful for mild-to-moderate pain, particularly at night. Safer for long-term use than NSAIDs, though not as effective for inflammatory coccydynia.
Neuropathic pain medications: In chronic cases where nerve irritation is a component, medications such as gabapentin or amitriptyline may be prescribed by a pain specialist. These are not first-line but can be effective for refractory coccydynia with nerve involvement.
Topical Treatments
NSAID gels (diclofenac gel, ibuprofen gel) applied directly over the coccyx provide local anti-inflammatory effect with minimal systemic absorption. Useful for patients who cannot take oral NSAIDs, and as an adjunct to oral medication.
Capsaicin cream — derived from chilli peppers — reduces pain sensation in the local nerve endings. Initially causes a burning sensation; consistent use over 2–4 weeks reduces local pain sensitivity. Not suitable for use on broken or irritated skin.
Corticosteroid Injections
A corticosteroid injection into the sacrococcygeal joint is one of the most effective non-surgical interventions for chronic coccydynia, particularly when inflammation is the primary driver of pain.
What it involves: Under X-ray or ultrasound guidance, a pain specialist or radiologist inserts a small needle into the sacrococcygeal joint and deposits a corticosteroid (typically triamcinolone or methylprednisolone) with a local anaesthetic. The procedure takes 15–20 minutes and is done as an outpatient.
Effectiveness: Studies report meaningful pain relief in 60–70% of patients. Pain reduction typically begins within 48–72 hours and peaks at 2–4 weeks. The effect usually lasts 3–6 months, and injections can be repeated (typically up to 3–4 times per year).
Risks: Short-term: local pain at the injection site (usually resolves in 24–48 hours), possible temporary increase in pain. Long-term: corticosteroid can weaken surrounding soft tissues with repeated injections — your pain specialist will advise on safe frequency limits.
Who is most suitable: Patients with chronic coccydynia (more than 6 months) who have not responded adequately to cushions, physiotherapy, and oral medications. The injection is most effective when pain is clearly originating from the sacrococcygeal joint (confirmed by diagnostic block).

Ganglion Impar Block
The ganglion impar is a cluster of nerve cells located at the front of the coccyx that carries pain signals from the coccyx and perianal region. A ganglion impar block involves injecting a local anaesthetic (with or without corticosteroid) into this nerve cluster.
This is a more advanced procedure than a sacrococcygeal joint injection and is typically performed by a pain specialist or interventional radiologist. It is reserved for patients with severe, refractory coccydynia who have not responded to joint injections and conservative treatment.
Effectiveness rates in the literature range from 45–75%, with some patients achieving pain relief for 6–12 months or longer.
Platelet-Rich Plasma (PRP) Injections
PRP is an emerging treatment in sports and musculoskeletal medicine. Your own blood is drawn, processed to concentrate platelets and growth factors, and injected into the injured area. For coccydynia, PRP aims to promote healing of the damaged sacrococcygeal joint and surrounding tissues.
Early evidence is promising but limited. PRP is significantly more expensive than corticosteroid injections ($800–1,500 per injection vs $300–600) and is not covered by most insurance plans. It may be worth considering for patients who have achieved only partial benefit from corticosteroid injections and wish to explore regenerative options before surgery.
Ergonomic and Lifestyle Modifications
Workplace Ergonomics
For office workers with coccyx pain, the right ergonomic setup dramatically reduces daily aggravating factors.
Chair selection: Your office chair must either have a coccyx cutout (specialist ergonomic chairs exist) or be used with a coccyx cushion. Standard office chairs — even expensive ergonomic ones — typically place significant pressure on the tailbone in a seated position.
Desk height: An incorrectly set desk height causes you to lean forward or slump, both of which increase coccyx pressure. Your monitor should be at eye level, your keyboard at elbow height, and your feet flat on the floor or on a footrest.
Mouse and keyboard position: Reaching for a mouse placed to the side causes lateral pelvic tilt that loads one side of the coccyx. Keep your mouse close and directly in front of you.
Phone and document holder: Looking down at documents on your desk or phone causes neck and upper back strain that compounds lower back and coccyx discomfort. Use a document holder at monitor height and a stand for your phone.
Driving Modifications
Driving is particularly aggravating for coccyx pain because the seat angle places the coccyx under pressure and the vibration of the vehicle constantly stimulates the sacrococcygeal joint.
Use a coccyx cushion in the car. Most users find a significant reduction in driving pain with a dedicated car cushion.
Adjust the seat angle. Reclining the seat slightly reduces pressure on the coccyx — but not so much that it compromises your ability to see the road safely.
Take breaks on long drives. Stop every 45–60 minutes, get out of the car, and walk for 2–3 minutes. This allows the coccyx to decompress and prevents cumulative aggravation.
Consider a coccyx cushion designed for car use — some models are specifically designed with a non-slip base and handle for automotive application.
Exercise Modifications
Exercise is important for overall health and circulation — but certain activities significantly aggravate coccyx pain.
Avoid:
- Cycling (the forward-leaning position and saddle pressure directly load the coccyx — even stationary bike at the gym is often problematic)
- Rowing machines (the seated, forward-lean position compresses the coccyx)
- Horse riding (the impact and saddle pressure are extremely aggravating)
- Sit-ups and crunches (the coccyx is pressed against the mat during the curl phase)
- Long-duration plank or push-up positions (prone coccyx loading)
Modify:
- Swimming — use a pull buoy between the legs to avoid the flutter kick that stresses the pelvic area; breaststroke kick should be gentle
- Walking — a flat, soft surface is fine; avoid uphill if it causes you to lean forward excessively
- Yoga — avoid forward folds while seated (use blocks under the hips), avoid deep seated twisting, modify prone poses with a pillow under the pelvis
Safe alternatives: Pilates (with appropriate modifications — see our pilates for coccyx pain guide), gentle stretching, swimming with pull buoy, light walking, and physiotherapy-prescribed exercises.
Diet and Bowel Management
Coccyx pain is frequently aggravated by bowel movements — particularly hard stools that require straining, which places enormous force on the coccyx through the pelvic floor attachments.
Prevent constipation: Eat adequate fibre (25–30g daily), drink sufficient water (1.5–2L daily), and stay physically active. These three factors are the foundation of bowel regularity.
Use a footstool during defecation: The squat position (elevated feet on a footstool, knees above hips) straightens the anorectal angle and significantly reduces straining. A small footstool placed in front of the toilet during defecation is one of the simplest and most effective bowel habit modifications for coccyx pain patients.
Avoid straining: If you consistently strain during bowel movements, discuss this with your GP or a pelvic health physiotherapist. Pelvic floor dysfunction may be contributing to bowel emptying difficulty.
Consider a peri bottle or bidet: Cleaning after bowel movements without wiping can reduce perianal irritation that aggravates the area around the coccyx.
Alternative and Complementary Therapies
Chiropractic and Osteopathy
Manual therapists with specific experience in treating coccydynia can perform gentle manipulation of the sacrococcygeal joint to address hypomobility (stuck joint). Gentle mobilisations — never aggressive adjustments — can improve joint mechanics and reduce pain.
Important cautions:
- Ensure your practitioner has specific experience treating coccydynia — general spinal adjustments may miss the specific mechanics of the tailbone
- Be clear about your coccyx pain during every visit — some patients report their practitioner not being aware of the coccyx involvement during treatment
- Avoid any high-velocity manipulation of the coccyx — the joint is too small and the tissues too sensitive for forceful adjustment
What to look for: A practitioner who discusses internal examination (with your consent) and explains specifically how they will approach the sacrococcygeal joint. Avoid any practitioner who dismisses the coccyx as the source of your pain.
Acupuncture and Dry Needling
Acupuncture — both traditional Chinese acupuncture and Western medical acupuncture — has evidence for managing chronic musculoskeletal pain conditions, including low back and pelvic pain. The evidence is not specific to coccydynia, but many patients report temporary reduction in pain following acupuncture sessions.
Dry needling of the surrounding gluteal and pelvic floor muscles can release trigger points that contribute to secondary muscle pain around the coccyx. This is typically performed by a physiotherapist trained in the technique.
Realistic expectation: Acupuncture provides pain relief for some patients but the effect is typically temporary (hours to days). It is not a standalone treatment for coccydynia but can be a useful adjunct to physiotherapy and cushion-based management.
Yoga Therapy
Yoga can be very helpful for coccyx pain — but only with the right teacher and the right modifications. The key principles:
- Avoid forward folds and seated poses without hip elevation
- Use blocks and props liberally to reduce the range of motion required
- Focus on gentle hip opener stretches (supta padangushthasana, gentle wind-relieving pose) rather than intense seated forward bends
- Avoid bhujangasana (cobra) and dhanurasana (bow) — prone back extensions compress the coccyx
A yoga teacher with experience in therapeutic yoga or prenatal/postpartum yoga will have the most appropriate knowledge for coccydynia modifications.
TENS Machines
A TENS (transcutaneous electrical nerve stimulation) machine delivers mild electrical currents through pads placed on the skin. For coccyx pain, pads are placed on either side of the tailbone and at the lower back.
TENS works through two mechanisms: gate control (the electrical signals compete with pain signals at the spinal cord level) and the release of natural endorphins at higher intensities.
Not all patients find TENS useful, but many report it as an effective adjunct during flare-ups, particularly at night when pain disturbs sleep. A basic TENS machine costs $30–80 and is a reasonable self-management investment if cushions and physiotherapy alone are not providing sufficient relief during acute periods.
When Surgery Becomes Necessary
Surgery for coccyx pain — called a coccygectomy — involves the partial or total removal of the coccyx. It is a significant procedure and a genuine last resort.
Who Is Considered for Coccygectomy
Surgery is considered when:
- At least 12 months of conservative treatment (cushions, physiotherapy, injections) has failed to provide adequate relief
- Imaging confirms a structural abnormality in the coccyx (fracture, dislocation, degenerative joint disease)
- Pain is severe enough to significantly impair daily function, work, or quality of life
- The patient has been assessed by a specialist who confirms the coccyx as the primary pain source
The Procedure
Coccygectomy is performed under general anaesthetic. The surgeon makes a small incision directly over the tailbone, detaches the attached muscles and ligaments, and removes the coccyx (or the portion that is damaged). The wound is closed with sutures.
Hospital stay: 1–3 days typically. Full recovery: 6–12 months for complete bone and soft tissue healing. The procedure is performed by spinal surgeons, colorectal surgeons, or orthopaedic surgeons with pelvic experience.
Effectiveness and Risks
The evidence for coccygectomy is limited by small study sizes and variable patient selection criteria. Generally:
- 60–80% of patients report meaningful long-term pain reduction after coccygectomy
- 15–25% report minimal or no improvement
- 5–10% report worsened pain or complications
Risks and complications:
- Infection (the surgical site is close to the bowel, and wound breakdown occurs in approximately 5–10% of cases)
- Persistent postoperative pain
- Altered sitting comfort even after healing
- Nerve injury causing chronic perineal numbness or hypersensitivity
- Bowel/bladder dysfunction (rare but documented)
- Prolonged recovery preventing return to work for 3–6 months
The mixed evidence and meaningful complication risk mean surgery should be a carefully considered last resort — not a treatment to rush toward. Patients should seek a second surgical opinion before proceeding.
Recovery from Coccygectomy
Postoperative recovery involves:
- Weeks 1–2: Strict off-loading, wound care, pain management
- Weeks 3–6: Gradual return to light activities; no sitting directly on the tailbone (use a cushion)
- Weeks 6–12: Introduction of gentle physiotherapy; return to desk work
- 3–6 months: Progressive return to normal activities and exercise
- 6–12 months: Continued bone healing; final functional outcome achieved
Patients report that the first 4–6 weeks are the most difficult — sitting is severely limited, wound care is required, and pain can be significant despite medication. A strong support system and workspace modification plan are essential before proceeding.
Recovery Timeline: What to Expect
Every patient's recovery is individual, but the following timeline provides a realistic framework:
| Phase | Timeframe | What to Expect | Treatment Focus |
|---|---|---|---|
| Acute | 0–4 weeks | Pain at its worst; sitting very limited | Rest, ice/heat, coccyx cushion, pain medication |
| Sub-acute | 4–12 weeks | Gradual pain reduction; physiotherapy most effective here | Manual therapy, targeted exercises, ergonomic modifications |
| Healing | 3–6 months | Meaningful improvement for most patients with conservative care | Continued physiotherapy, injection if not progressing |
| Chronic | 6–12 months | If pain persists without improvement, escalate to specialist and injection options | Pain specialist review, imaging, consider injection or second opinion |
| Surgical | 12+ months | Surgery considered only if all conservative options exhausted | Surgical consultation, coccygectomy if appropriate |
Key message: Most coccyx pain improves with conservative treatment. If you are more than 8 weeks into coccyx pain without any improvement, you are likely not receiving the right treatment — seek a specialist pelvic physiotherapist or a coccyx-aware pain specialist.
Frequently Asked Questions
What causes coccyx pain?
Coccyx pain (coccydynia) is caused by trauma such as falls or childbirth, prolonged sitting on hard surfaces, joint hypermobility or hypomobility, degenerative joint changes, and referred pain from the sacroiliac joint or pelvic floor. The most common cause is a direct fall onto the tailbone.
How long does coccyx pain typically last?
Acute coccyx pain from a bruise or mild sprain typically resolves within 4–12 weeks with conservative treatment. More significant injuries such as fractures may take 6–12 months. Chronic coccydynia (pain lasting more than 3 months) may persist for years without proper treatment.
Does sitting make coccyx pain worse?
Yes. Sitting — especially on hard surfaces — places direct pressure on the coccyx and is the primary aggravating factor for most people with coccydynia. Using a coccyx cushion with a U-shaped rear cutout eliminates this pressure and is the single most effective home modification for coccyx pain.
What non-surgical treatments work best for coccyx pain?
The most effective non-surgical treatments are: (1) a quality coccyx cushion, (2) physiotherapy with manual coccyx mobilisation, (3) targeted exercises including pelvic floor work, (4) corticosteroid or platelet-rich plasma injections for refractory pain, and (5) lifestyle modifications to reduce sitting pressure. Most patients achieve significant relief with these approaches combined.
When is surgery needed for coccyx pain?
Surgery (coccygectomy — partial or total removal of the coccyx) is considered only after 12+ months of failed conservative treatment. It is a last resort reserved for patients with severe, disabling pain that has not responded to cushions, physiotherapy, injections, and other non-surgical interventions.
Can a coccyx cushion really help tailbone pain?
Yes. A coccyx cushion with a U-shaped rear cutout eliminates direct pressure on the tailbone when sitting. This allows inflamed tissues to heal and prevents ongoing irritation. Look for high-density memory foam at least 3 inches thick with a genuine rear cutout (not just a notch). The Everlasting Comfort Seat Cushion and ComfiLife Gel are top-recommended options.
What exercises help coccyx pain?
Exercises that help coccyx pain include: pelvic tilts (to mobilise the sacrococcygeal joint), knee-to-chest stretches (to release gluteus maximus tension), piriformis stretches (side-lying), gentle cat-cow breathing (for spinal mobility), and pelvic floor relaxation exercises. Avoid exercises that place direct pressure on the coccyx such as roll-ups, seated forward bends, or prolonged prone positioning.
Are injections effective for coccyx pain?
Corticosteroid injections into the sacrococcygeal joint provide meaningful relief in approximately 60–70% of patients with chronic coccydynia, particularly when inflammation is a primary driver of pain. The effect typically lasts 3–6 months and can be repeated. More recently, platelet-rich plasma (PRP) injections have shown promise in early studies for longer-lasting results in cases where steroid injections have been only partially effective.
Sources & Methodology
This article is based on a combination of clinical evidence, physiotherapy research, and Mat's personal experience managing coccyx pain over 9 years. Key sources and references include:
- British Journal of Sports Medicine — systematic reviews on core stabilisation and musculoskeletal pain management
- Journal of Orthopaedic & Sports Physical Therapy — clinical guidelines for coccydynia assessment and treatment
- Cochrane Database of Systematic Reviews — evidence for physiotherapy interventions in chronic pain
- American Physical Therapy Association — clinical practice guidelines for pelvic floor dysfunction
- Pelvic Health Alliance Australia — anatomy and assessment protocols for coccydynia and pelvic floor conditions
- Archives of Physical Medicine and Rehabilitation — research on corticosteroid injection efficacy for sacrococcygeal joint pain
This article is for informational purposes only and does not constitute medical advice. Coccyx pain can have serious underlying causes. Consult a qualified healthcare provider — ideally a pelvic physiotherapist or coccyx-specialist doctor — before beginning any new treatment programme.
About the author: Mat spent 9 years managing coccyx pain personally before finding what actually worked. He writes about coccyx pain to help others avoid the same delayed diagnosis and ineffective treatment path he experienced. This site is reader-supported — we may earn a commission from Amazon links, at no extra cost to you.
Get the Exact System That Reduced My Pain by 90%+
30+ pages of exercises, methods, and the complete program that helped me go from agony to pain-free.
Get My Coccyx Relief SystemInstant download • 30-day money-back guarantee