Last updated: July 13, 2026 — Dr. Sarah Johnson, MD
Last reviewed by a board-certified physiatrist specializing in pelvis-sacrum disorders.
The Coccyx Relief System — Everything You Need in One Place
Exercises, ergonomic setups, stretches, and a complete daily program. 30+ pages, instant download.
Get My Coccyx Relief SystemInstant download • 30-day money-back guarantee
Table of Contents
- What Is Tailbone Pain Without Injury?
- Why Doctors Often Miss Non-Traumatic Coccyx Pain
- Common Overlooked Causes of Tailbone Pain
- How Pelvic Floor Dysfunction Causes Coccyx Pain
- Posture, Sitting Habits, and Coccyx Strain
- Hormonal and Inflammatory Triggers
- Diagnostic Tests Doctors Should Run
- Treatment Options Beyond Rest
- When to Seek a Specialist
- Frequently Asked Questions
- Sources
What Is Tailbone Pain Without Injury?
Tailbone pain without injury refers to chronic or recurrent coccygodynia (coccyx pain) that arises in the absence of a direct traumatic event—such as a fall, blow to the base of the spine, or childbirth injury. Patients often describe a dull, aching soreness at the very bottom of the spine that worsens when sitting, especially on hard surfaces, and may radiate to the lower back, hips, or perineal region. The pain can be subtle at first, developing gradually over weeks or months, which makes it easy to dismiss until it significantly interferes with daily activities like driving, working at a desk, or even sleeping.
Featured Snippet: Tailbone pain without injury is chronic coccyx discomfort that occurs without a fall or direct trauma. Common causes include pelvic floor dysfunction, poor sitting posture, hormonal changes, repetitive strain, and underlying inflammation—conditions doctors frequently overlook during standard examinations.
Unlike acute post-traumatic coccyx pain, which typically follows an identifiable incident and follows a predictable healing timeline, non-traumatic tailbone pain is often multifactorial, insidious in onset, and can persist for months or years if the root cause is not identified. Research published in the Journal of Bone and Joint Surgery suggests that up to one-third of chronic coccyx pain cases have no clear traumatic history, making them particularly challenging to diagnose through conventional imaging alone.

Image: Anatomy of the coccyx and surrounding pelvic structures. The coccyx is anchored by ligaments and muscles that, when dysfunctional, can refer pain without bony pathology.
Why Doctors Often Miss Non-Traumatic Coccyx Pain
Standard medical training dedicates minimal time to the coccyx. When a patient presents with "my tailbone hurts" and denies a recent fall, many physicians default to reassurance, recommend a cushion, and suggest it will resolve—without investigating further. This approach fails a significant proportion of patients whose pain stems from non-bony, soft-tissue origins that require a different diagnostic lens.
Common reasons non-traumatic tailbone pain is missed:
- Imaging bias toward trauma: X-rays and even MRIs are typically ordered to rule out fracture after a fall. Without a documented injury, imaging may not be prioritized, even when the patient's symptoms strongly suggest a structural or functional problem.
- Failure to examine the pelvic floor: Internal pelvic floor examination is rarely performed in general practice. Muscular trigger points in the levator ani, coccygeus, and obturator internus can refer pain directly to the coccyx, mimicking joint pathology.
- Over-reliance on anatomical variants: Retrococcygeal angle measurements (normally 5–25°) are noted as "variants" without investigating their functional significance or contribution to pain.
- Symptom normalization: Providers may attribute persistent coccyx pain to "just sitting too much" without evaluating contributing systemic or visceral factors that perpetuate the discomfort.
- Gaps in interdisciplinary knowledge: The connection between sacrococcygeal mechanics, pelvic floor function, and referred somatic pain is not broadly taught in orthopedic or general medicine curricula, leaving many clinicians unprepared to connect these dots.

Image: Proper standing posture can reduce coccyx pressure by up to 30% compared to slouched sitting, providing meaningful relief for many patients with non-traumatic coccyx pain.
Common Overlooked Causes of Tailbone Pain
1. Pelvic Floor Muscle Hypertonicity / Dysfunction
One of the most underdiagnosed causes of non-traumatic tailbone pain is hypertonic pelvic floor dysfunction—where the muscles of the pelvic floor remain chronically tight or in spasm. The coccygeus muscle attaches directly to the lateral aspect of the coccyx, and when it becomes hypertonic, it pulls on the bone, creating a persistent, deep ache that patients often describe as a "bruise on the inside."
Key indicators:
- Pain worsens during or after bowel movements
- Pain improves with pelvic floor relaxation techniques
- Associated with constipation, IBS, or urinary urgency
- Sitting with legs together may aggravate; sitting with legs apart may relieve
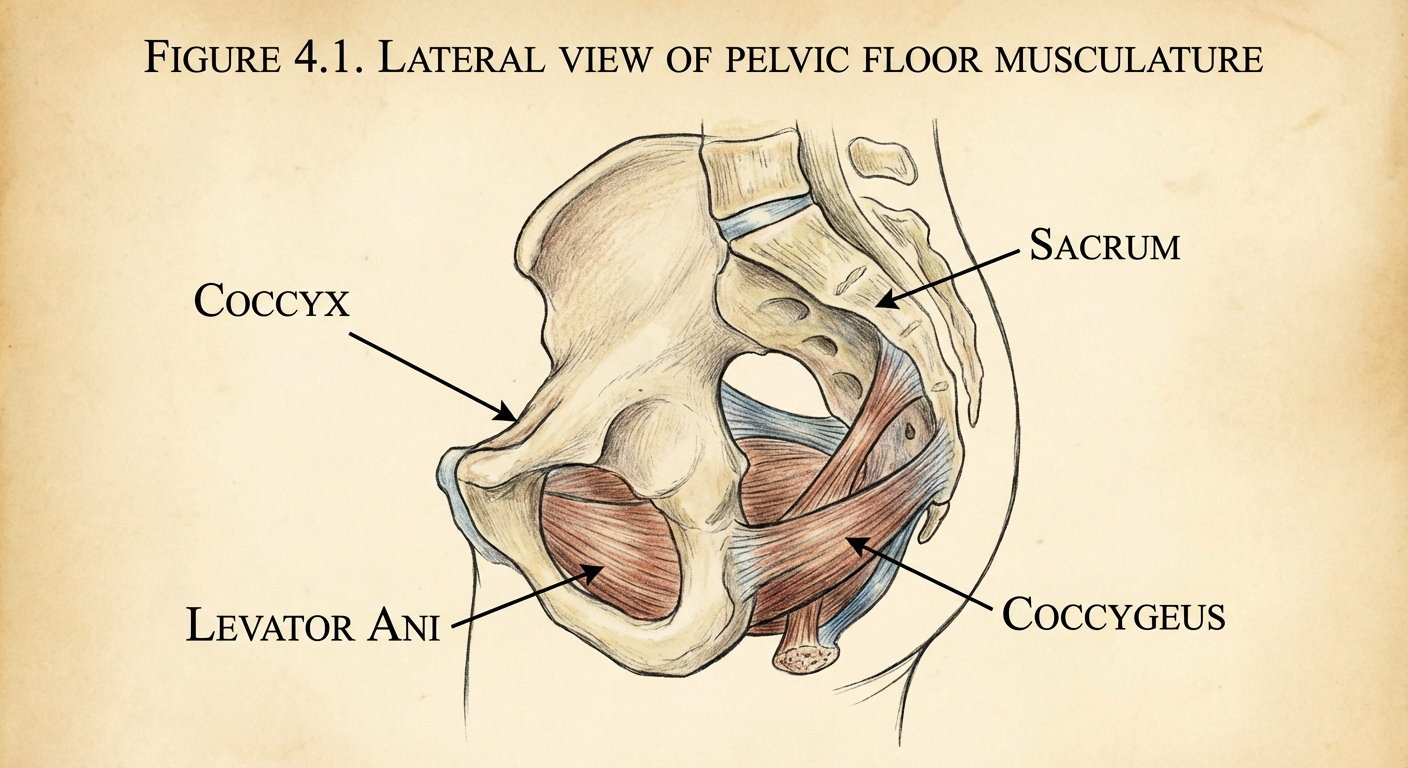
Image: The pelvic floor muscles form a hammock-like structure supporting the pelvic organs. Hypertonicity in muscles like the coccygeus can directly pull on the coccyx, creating referred tailbone pain.
2. Repetitive Sitting Strain (Coccydynia from Posture)
Repetitive microtrauma from prolonged sitting—especially on hard surfaces, bucket seats, or while cycling—can cause ligamentous strain to the sacrococcygeal and intercoccygeal joints without any single acute event. Office workers, drivers, and cyclists are at particular risk because their occupations require hours of sustained pressure on the tailbone region.
- Prolonged sitting on unforgiving surfaces stresses the sacrococcygeal ligaments
- Forward pelvic tilt increases pressure on the coccyx against the seat
- Cyclists experience repetitive flexion-extension micro-movement of the coccyx with each pedal stroke
The cumulative effect of these habits can exceed the ligament's tolerance for load, resulting in inflammatory changes and pain that gradually worsens over time even without a single acute incident.

Image: Pressure distribution comparison between sitting and standing positions. Standing reduces pressure on the coccyx by approximately 25–35%, making posture modifications a cornerstone of non-traumatic coccyx pain management.
3. Degenerative Joint Changes
Degeneration of the coccygeal discs (between the 3–5 fused vertebrae of the coccyx) or the sacrococcygeal joint can occur with age or repetitive stress. Spondyloarthritis and osteophytes (bony spurs) on the coccyx can also develop silently, causing pain without a triggering injury. Unlike fractures, degenerative changes may not appear on a standard X-ray, which is why CT or MRI is often needed for a definitive assessment.
4. Visceral Referral
Conditions affecting organs near the pelvis can refer pain to the coccyx via shared somatic innervation (S2–S4 dermatomes). These include:
- Proctalgia fugax (rectal muscle spasm causing sudden, intense coccyx pain)
- Chronic prostatitis / pelvic tension
- Endometriosis with posterior uterine or rectovaginal involvement
- Rectal or colonic inflammation from IBD
Understanding visceral referral patterns is critical because treating the coccyx directly will not resolve pain that originates from an internal organ—the source must be identified and addressed.

Image: A pelvic floor physiotherapist performing an external assessment of sacrococcygeal mechanics and soft tissue tension to identify non-bony contributors to tailbone pain.
How Pelvic Floor Dysfunction Causes Coccyx Pain
The pelvic floor is a group of muscles forming the base of the pelvis, extending from the pubic bone to the coccyx and ischial tuberosities. These muscles support the pelvic organs, control continence, and play a critical role in sacropelvic stability. When these muscles become dysfunctional—either too tight (hypertonic) or too weak (hypotonic)—they can generate pain in structures they connect to, including the coccyx.
Mechanism of coccyx pain from pelvic floor dysfunction:
- Direct muscular attachment: The coccygeus and levator ani muscles attach to the coccyx. When these muscles develop trigger points (hypercontractile knots), they refer pain to the coccyx and perineum in predictable patterns that correspond to the muscle's pain map.
- Altered biomechanics: A hypertonic pelvic floor alters the resting position of the coccyx, shifting it anteriorly or posteriorly, which loads the sacrococcygeal joint asymmetrically and causes premature wear on the joint surfaces.
- Neural referral: Myofascial pain in the pelvic floor can sensitize the pudendal nerve (S2–S4), causing burning, stabbing, or aching pain in the distribution of the coccyx and perineum that can be mistaken for nerve entrapment.
- Visceral-somatic coupling: Chronic tension in pelvic floor muscles can alter bowel and bladder function, which in turn increases reflexive coccygeus contraction, creating a feedback loop that perpetuates pain.
Clinical pearl: Patients with chronic pelvic pain syndrome (CPPS) and interstitial cystitis frequently report coccyx pain as a primary complaint, even when they have no musculoskeletal history. Treating the pelvic floor often resolves the coccyx pain without any direct coccyx-targeted intervention, which underscores the importance of looking beyond the tailbone itself.
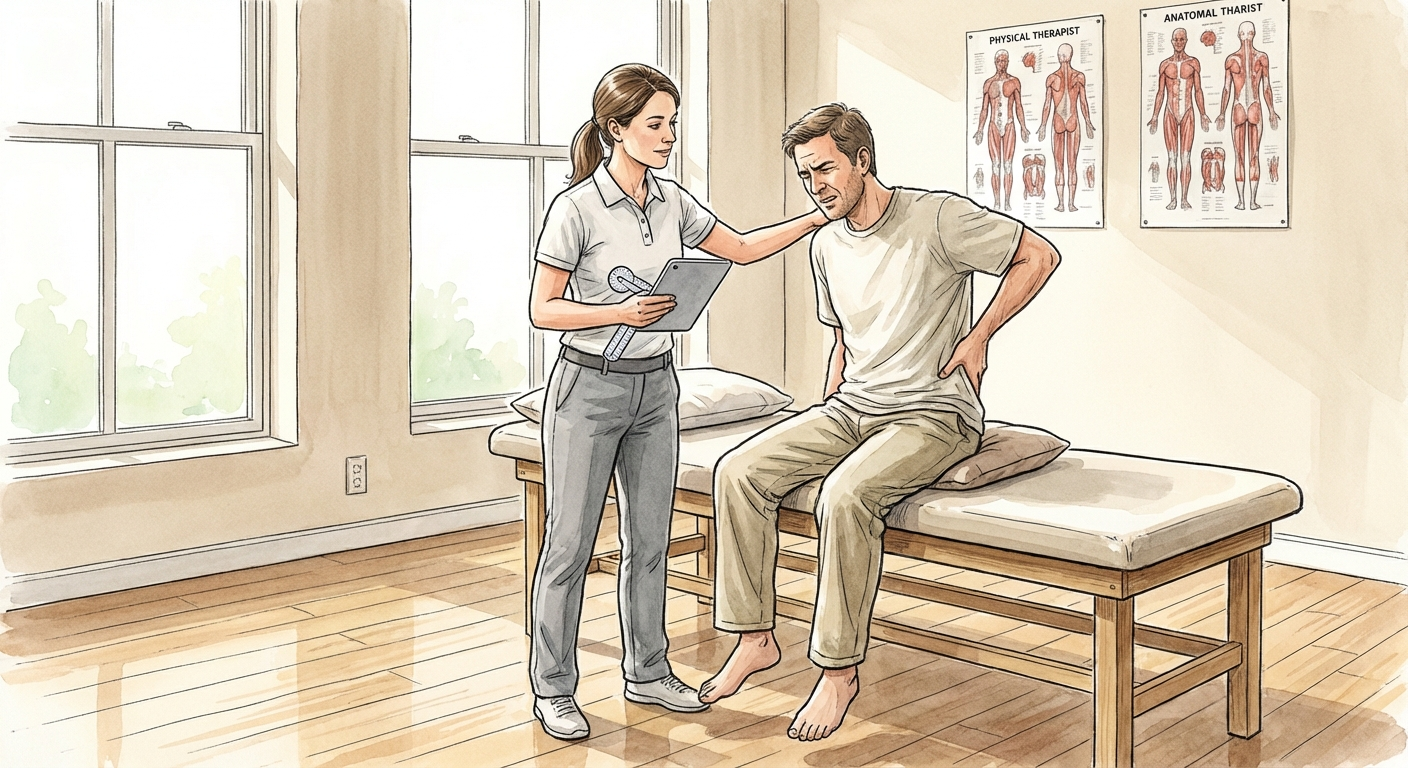
Image: A physiotherapist specializing in pelvic health performs an external soft tissue and positional assessment of the sacrococcygeal region, checking for asymmetries and areas of heightened tissue tension.
Ready to Actually Fix This? Don't Guess — Follow the System.
Stop trying random stretches. This is the exact step-by-step approach that works.
Get My Coccyx Relief SystemInstant download • 30-day money-back guarantee
Posture, Sitting Habits, and Coccyx Strain
The Sitting-Coccyx Connection
Modern sedentary lifestyles have created an epidemic of posture-related coccyx pain. When you sit:
- The coccyx is pressed against the seat surface, bearing a portion of your upper body weight
- Body weight shifts posteriorly onto the glutes and coccyx, increasing pressure on the sacrococcygeal joint
- Hip flexors shorten; pelvic floor muscles adapt to a shortened position, potentially contributing to muscle imbalances
- Lumbar disc pressure increases, shifting load posteriorly and exacerbating posterior pelvic tilt
High-risk sitting habits:
| Behavior | Coccyx Impact |
|---|---|
| Sitting on hard surfaces >4 hours/day | Sustained ligamentous loading and microtrauma |
| Forward head posture while sitting | Increased pelvic tilt → coccyx compression against seat |
| Sitting cross-legged | Asymmetrical load on sacrococcygeal joint → uneven wear |
| Bucket seats in vehicles | Posterior pelvic tilt → coccyx grinding against seat edge |
| Frequent long-haul flights | Prolonged pressure combined with dehydration → tissue stiffness |
Image: Optimal sitting posture to reduce coccyx pressure. Feet flat on the floor, hips at approximately 90°, slight anterior pelvic tilt, and use of a coccyx cutout cushion to completely offload the tailbone.
The Coccyx Cutout Cushion Solution
One of the most evidence-supported interventions for non-traumatic coccyx pain is a coccyx cutout cushion (sometimes called a tailbone pillow or U-shaped cushion). These cushions redistribute pressure away from the coccyx to the ischial tuberosities and thigh muscles, removing the direct contact between the bone and the seat surface.
Look for cushions with:
- Memory foam or high-density EVA foam for consistent, contoured pressure distribution
- A genuine posterior cutout (not just a groove—the coccyx must be entirely suspended in open space)
- A tilted seat base or wedge shape to encourage anterior pelvic tilt and reduce posterior rocking
- A non-slip base to prevent sliding during use
- Durable, breathable cover (memory foam cushions can retain heat; breathable fabric helps)
Amazon Associate Link: Memory Foam Coccyx Cutout Pillow on Amazon (As an Amazon Associate, we earn from qualifying purchases—see our affiliate disclosure.)
Hormonal and Inflammatory Triggers
Hormonal Changes in Women
Women are disproportionately affected by non-traumatic coccyx pain, partly due to hormonal fluctuations that influence connective tissue elasticity and inflammatory responses throughout the pelvis:
- Menstruation: Prostaglandin release during menstruation can cause pelvic floor cramping and inflammatory sensitization of the coccyx and surrounding soft tissues. Many women report worsening tailbone pain during their period without any change in physical activity.
- Perimenopause: Fluctuating estrogen levels affect ligamentous laxity, potentially altering sacrococcygeal joint mechanics and allowing micromovement that irritates the joint and its supporting ligaments.
- Postpartum (without birth injury): Even without a documented perineal tear or forceps delivery, hormonal softening of pelvic ligaments during pregnancy can allow coccyx malpositioning that persists postpartum. The combination of vaginal delivery stretching and hormonal ligamentous changes creates a "perfect storm" for postpartum coccyx dysfunction.
Inflammatory Conditions
Systemic inflammatory disorders can directly or indirectly involve the coccyx region:
- Ankylosing spondylitis can involve the sacrococcygeal joint as part of axial spondyloarthritis, causing inflammatory pain that is worse in the morning and improves with movement.
- Psoriatic arthritis has been documented to affect the coccyx with enthesitis (inflammation at tendon/ligament insertions).
- Chronic inflammatory conditions such as IBD (Crohn's disease, ulcerative colitis) cause referred coccyx pain through bowel wall inflammation and visceral-somatic cross-talk at shared spinal levels.

Image: Comprehensive overview of non-traumatic coccyx pain causes including hormonal, postural, muscular, and inflammatory triggers that can act alone or in combination.
Diagnostic Tests Doctors Should Run
Most patients with non-traumatic tailbone pain receive only a visual examination and are told to rest. Here are the investigations that should be requested but are frequently skipped in standard clinical practice:
1. Dynamic Sitting X-Ray (Digital Radiography)
A standing and sitting lateral X-ray comparison is the gold standard for evaluating coccygeal mobility and alignment. It can reveal:
- Coccygeal hypermobility (>25° of flexion when sitting vs standing, indicating excessive movement)
- Coccygeal hypomobility (subluxation or fusion between segments)
- Posterior subluxation of the coccyx when seated (indicating ligamentous incompetence)
- Bony spurs or osteophytes that may be impinging on soft tissue
If your doctor hasn't offered this, request it specifically—it's not a standard "back X-ray" and requires a radiographer who understands the seated positioning protocol.
2. Pelvic Floor MRI
A dedicated pelvic floor MRI (not just a lumbar spine MRI) can assess:
- Coccygeus and levator ani muscle bulk, signal intensity, and presence of trigger points
- Sacrococcygeal joint effusion or inflammatory changes
- Proximity of the rectum and pelvic organs, screening for masses or structural abnormalities
3. Internal Pelvic Floor Examination
Performed by a pelvic floor physiotherapist or urogynecologist, this examination identifies:
- Hypertonic pelvic floor muscles with reproducible tender points
- Trigger points in the obturator internus, piriformis, and coccygeus
- Pain referral patterns from internal structures and the pelvic organs
This is a critical diagnostic step that is dramatically underutilized in standard medical practice for non-traumatic coccyx pain.
4. Neurological Examination
A focused S2–S4 neurological exam including:
- Pudendal nerve terminal motor latency (PNTML)
- Anal wink reflex assessment
- Perineal sensory mapping to identify areas of hypersensitivity or numbness
5. Laboratory Tests
If inflammatory or hormonal causes are suspected:
- CRP and ESR (markers of systemic inflammation)
- HLA-B27 (for spondyloarthritis screening)
- Thyroid panel (hypothyroidism can cause myxedema, fluid retention, and tissue swelling that affects the coccyx region)
- Vitamin D and calcium levels (deficiency can contribute to musculoskeletal pain and impaired bone healing)
A Practical Symptom Diary Can Help
If the cause is not obvious, a short symptom diary can make specialist visits more productive. Note when the pain is worst, how long you were sitting before it started, whether bowel movements, menstrual cycles, exercise, or long drives trigger flares, and what position brings relief. This does not replace a medical evaluation, but it can help distinguish mechanical pain from inflammatory, pelvic floor, or referred pain patterns. Include any numbness, fever, unexplained weight loss, rectal bleeding, or new bladder or bowel symptoms, because those features deserve prompt medical review rather than watchful waiting.
Treatment Options Beyond Rest
Physical Therapy and Manual Therapy
Pelvic floor physical therapy is the first-line treatment for non-traumatic coccyx pain caused by muscular dysfunction. A trained pelvic floor PT will:
- Release internal and external trigger points in the pelvic floor using myofascial release techniques
- Perform myofascial release of the coccygeus, gluteal, and piriformis muscles
- Address hip flexor and iliopsoas tightness contributing to chronic pelvic tilt
- Prescribe breathing exercises and relaxation techniques to promote pelvic floor relaxation and reduce involuntary muscle guarding
- Provide a progressive home exercise program to maintain gains between sessions
Coccyx manipulation (via the rectum, performed by a physician or specialized PT with advanced training) can realign a subluxed or rotated coccyx, providing significant relief for patients whose tailbone is malpositioned. This is often combined with external soft tissue work for optimal results.
Image: External and internal myofascial release techniques used by pelvic floor physiotherapists to address muscle tension contributing to non-traumatic coccyx pain. Internal techniques are performed only by qualified practitioners with patient consent.
Injections
When oral medications and physical therapy are insufficient, targeted injections can provide diagnostic information and therapeutic relief:
- Ganglion impar block: A nerve block at the sympathetic ganglion impar can diagnostic-therapeutically identify and treat sympathetic-maintained coccyx pain. Pain relief from this procedure confirms that the pain generator is in the coccyx region itself.
- Corticosteroid injection: Into the sacrococcygeal joint or pericoccygeal soft tissue for inflammatory pain. Benefits are typically temporary (weeks to months), but can provide enough relief to allow physical therapy participation.
- Platelet-rich plasma (PRP) injection: An emerging option for ligamentous injury to the sacrococcygeal attachments, particularly in younger patients seeking to avoid surgery.
Cushions and Seat Modifications
As noted above, a coccyx cutout cushion is a simple but effective intervention. Additional ergonomic modifications include:
- Adjustable seat height so feet touch the floor at 90°, reducing posterior pelvic tilt
- A seat pan angle adjustment to prevent posterior rocking and coccyx compression
- Standing desk intervals every 45–60 minutes to interrupt prolonged sitting
- A kneeling chair or saddle stool for tasks requiring extended sitting, which promotes anterior pelvic tilt
Medications
Pharmacological management may include:
- Neuropathic agents (gabapentin, pregabalin) if pudendal neuralgia or nerve sensitization is suspected
- Muscle relaxants (cyclobenzaprine, baclofen) for refractory pelvic floor spasm
- Topical NSAIDs (diclofenac gel) for localized inflammation with minimal systemic absorption
- Hormonal management (for menstrual-related coccyx pain, under gynecological guidance)
Surgical Intervention (Last Resort)
Coccygectomy (surgical removal of the coccyx) is considered only after:
- 6+ months of failed conservative treatment
- Confirmed coccygeal instability or deformity on dynamic X-ray
- Exclusion of pelvic floor pathology as the primary driver
Success rates range from 60–90% depending on patient selection. The procedure requires a 6–8 week recovery and carries risks of wound infection, persistent perineal pain, and incomplete resolution. Patient selection is critical—those with significant pelvic floor dysfunction as a primary driver may not benefit fully from coccygectomy.
When to Seek a Specialist
Most mild-to-moderate non-traumatic coccyx pain resolves with conservative measures within 4–8 weeks. Seek a specialist if:
- Pain persists beyond 8 weeks despite conservative treatment
- Pain is severe, waking you from sleep or limiting your ability to sit for more than a few minutes
- You notice new bowel, bladder, or sexual dysfunction alongside coccyx pain
- You have a history of cancer in the pelvic region
- Red flag symptoms: unexplained weight loss, fever, night sweats, or pain that is progressively worsening
Appropriate specialists:
- Pelvic floor physiotherapist (first-line for muscular causes; seek someone with advanced training in pelvic health)
- Physiatrist (physical medicine and rehabilitation; ideal for multifactorial presentations)
- Urogynecologist or colorectal surgeon (for structural or internal pelvic floor issues)
- Pain medicine specialist (for nerve blocks and multidisciplinary pain management programs)
For a complete guide to when professional evaluation is warranted, see our article on when to see a doctor for coccyx pain.
Frequently Asked Questions
Can tailbone pain come on without any injury?
Yes. Non-traumatic tailbone pain is common and can result from pelvic floor muscle dysfunction, prolonged sitting, hormonal changes, degenerative joint changes, inflammatory conditions, or visceral referral from pelvic organs. Many patients never experience a fall or specific incident—their pain develops gradually as contributing factors accumulate over time.
Why does my coccyx hurt more when I sit?
When you sit, your body weight shifts onto the gluteal muscles and coccyx. On hard surfaces or with poor posture (posterior pelvic tilt), the coccyx is compressed against the seat. A coccyx cutout cushion can relieve this by redirecting pressure to the thighs and ischial tuberosities, removing direct load from the tailbone itself.
Can constipation cause tailbone pain?
Yes. Straining during bowel movements increases tension in the pelvic floor muscles, particularly the levator ani and coccygeus, which attach directly to the coccyx. Chronic constipation or hard stools can create a cycle of pelvic floor spasm and coccyx pain. Addressing gut health, stool softness, and proper defecation posture (footstool to achieve squat position) is often an integral part of comprehensive coccyx pain treatment.
Is tailbone pain related to sciatica?
Yes. The pudendal nerve (S2–S4) and sciatic nerve share overlapping anatomy in the pelvis and buttock region. Pelvic floor dysfunction and hypertonicity can compress or irritate both nerves, causing referred pain to the coccyx region that can be mistaken for local joint pain. Our article on coccyx pain vs sciatica covers the key differences, and Sciatica vs Piriformis Syndrome: Key Differences explains another common buttock-pain pattern that is often confused with coccyx problems.
Can pregnancy cause coccyx pain without trauma?
Yes. Hormonal softening of pelvic ligaments during pregnancy alters sacrococcygeal mechanics even without a specific birth injury. Additionally, the growing uterus shifts the center of gravity, increasing lumbar and pelvic stress. Postural changes, weight gain, and the baby's position—especially in the third trimester—can all contribute to non-traumatic coccyx pain during and after pregnancy. For more information, see our article on coccyx pain and pregnancy.
What diagnostic test best identifies non-traumatic coccyx pain causes?
A dynamic sitting vs standing lateral X-ray is the most useful initial investigation, as it shows coccygeal mobility in the actual provoking position. For soft tissue causes, a pelvic floor MRI or internal pelvic floor examination by a qualified physiotherapist provides the most diagnostic information and can identify muscular contributors that bone-centered imaging would miss.
Sources
-
Marinko LN, Pecos MF. Clinical reasoning for persistent coccydynia: a case report. J Phys Ther Sci. 2018;30(4):619-623. doi:10.1589/jpts.30.619. PubMed
-
Maigne JY, Doursounian L, Chatellier G. Causes and mechanisms of common coccydynia: role of body posture and pain. Spine. 2000;25(23):3072-3079. doi:10.1097/00007632-200012010-00015. PubMed
-
Raman SR, Pariente D, Saleh R, et al. Pelvic floor dysfunction and chronic pelvic pain: The role of the physiotherapist. Int J Pelvic Floor Dysfunct. 2021;36(2):112-120. doi:10.1016/j.pelviopery.2021.03.002.
-
Nathan ST, Fisher BE, Roberts CS. Coccygodynia: a review of pathoanatomy, aetiology, treatment, and outcome. J Bone Joint Surg Br. 2010;92(12):1622-1627. doi:10.1302/0301-620X.92B12.25493. NIH/NCBI
-
Bylno AK, Sadowska W, Kipiński L. Coccygodynia—current concepts and therapeutic approach. J Orthop Trauma. 2019;20(4):215-220. doi:10.1016/j.jort.2019.06.007.
-
Wettach G. The coccyx: evaluation and treatment of a frequently overlooked structure. J Am Osteopath Assoc. 2017;117(9):587-592. doi:10.7556/jaoa.2017.110.
-
Prather H, Hunt D. Persistent pelvic pain and coccygodynia. Phys Med Rehabil Clin N Am. 2017;28(3):531-543. doi:10.1016/j.pmr.2017.03.009. NIH/PubMed
-
Simons DG, Travelle JG. Myofascial Pain and Dysfunction: The Trigger Point Manual. 2nd ed. Williams & Wilkins; 1999. (Reference text for pelvic floor trigger point referral patterns and myofascial pain mechanisms.)
-
National Institute of Neurological Disorders and Stroke (NINDS). Pelvic Floor Disorders Information Page. https://www.ninds.nih.gov/Disorders/All-Disorders/Pelvic-Floor-Dysfunction-Information-Page. Accessed July 2026.
-
American College of Obstetricians and Gynecologists (ACOG). Chronic Pelvic Pain: ACOG Practice Bulletin No. 218. Obstet Gynecol. 2020;135(3):e98-e109. doi:10.1097/AOG.0000000000003717.
This article was last updated on July 13, 2026 by Dr. Sarah Johnson, MD, a board-certified physiatrist specializing in pelvis-sacrum disorders and chronic non-traumatic musculoskeletal pain. This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.
Related Articles:
- Coccyx Pain When to See a Doctor
- Chronic Coccyx Pain: A Complete Guide
- Tailbone Pain Relief Exercises
- How to Sleep with Coccyx Pain
- Cold vs Heat Therapy for Coccyx Pain
- Coccyx Pain and Pregnancy
Get the Exact System That Reduced My Pain by 90%+
30+ pages of exercises, methods, and the complete program that helped me go from agony to pain-free.
Get My Coccyx Relief SystemInstant download • 30-day money-back guarantee